Myocarditis after COVID-19 Vaccination versus SARS-CoV2 Infection: Latest UK Study in Context
Stratified Analysis by Age and Sex reveals risk of vaccination may be greater than risk of SARS-CoV2 infection

BACKGROUND (latest study in context)
The recent preprint publication this month from Thailand (prospective study of myocarditis in adolescents after BNT126b2 vaccination) generated much interest amongst scientists, physicians, and general public alike. It has now been formally published in final form. My critique of the study from Thailand suggests it was deeply flawed. However, the intended methodology was commendable: it was the first study to prospectively evaluate all adolescents with baseline physical exam, EKG, echocardiogram (ultrasound of the heart), and important cardiac biomarkers (e.g., high sensitivity troponin). All students were then followed with repeated evaluation as above on day 3 and 7 after BNT162b2 (Pfizer) Dose 2. One case of symptomatic myocarditis was confirmed by cardiac MRI (CMR), while the students with asymptomatic suspected subclinical myocarditis did not have confirmation CMR (apparently due to budget constraints per my correspondence with the authors). That no such study was ever conducted, any demanded, in the USA by CDC and FDA prior to approval of COVID-19 vaccines is deplorable. The conspicuous absence of such a study in USA reflects either gross incompetence, willful negligence, or intentional data manipulation to advance an agenda.
[For alternate perspectives on the study from Thailand, see review by Dr. Vinay Prasad and Dr. Anish Koka.]
Reports of Vaccine Associated Myocarditis (VAM) first surfaced around April 2021 from Israel. In the US, CDC continued to rely almost exclusively upon data from Vaccine Adverse Events Reporting System (VAERS), repeatedly asserting in 2021 that the risk of VAM was low and most cases were generally mild. Since Fall 2021, however, numerous peer reviewed studies started surfacing suggesting that VAERS was underestimating the risk, and that there was a statistical association of VAM with mRNA COVID-19 vaccines (probably greater with mRNA-1273 COVID-19 vaccination). CDC’s initial calculations of the risks and benefits of COVID-19 vaccination were based upon aggregate endpoints across all ages. This obfuscated the anecdotal evidence from VAERS that seemed to suggest the risk of VAM was greater in adolescents and young adults, and perhaps more in males than in females. Additionally, COVID-19 infection carries much higher morbidity and mortality in elderly than in children and young adults.

Myocarditis data from VAERS in the US reveals 51,566 reports of myocarditis, pericarditis (or both). The actual number could be several times greater than the cases reported in VAERS via passive surveillance. The CDC and FDA ought to have conducted a more aggressive post market surveillance campaign to monitor the severe adverse events after COVID-19 vaccination.

RISK STRATIFICATION: SUBGROUP ANALYSIS BY AGE AND SEX
In one of the first stratified analyses of myocarditis after COVID-19 vaccination, Patone et al. published a comprehensive study from England in Dec 2021. This study included 38,615,491 adults from England who had received at least one dose of either ChAdOx1 (n = 20,615,911), BNT162b2 (n = 16,993,389) or mRNA-1273 (n = 1,006,191) between 1 December 2020 and 24 August 2021. Of these, 32,095,748 had received two doses of either ChAdOx1 (n = 19,754,224, 95.8%), BNT162b2 (n = 11,972,733, 70.5%) or mRNA-1273 (n = 368,791, 36.7%). COVID-19 vaccines were approved in those 16 years and older, so the study did not evaluate children and adolescents. (Subsequent studies including these younger cohorts have been previously reviewed in great detail here by myself). Baseline characteristics of the study population are as below in Table 1.
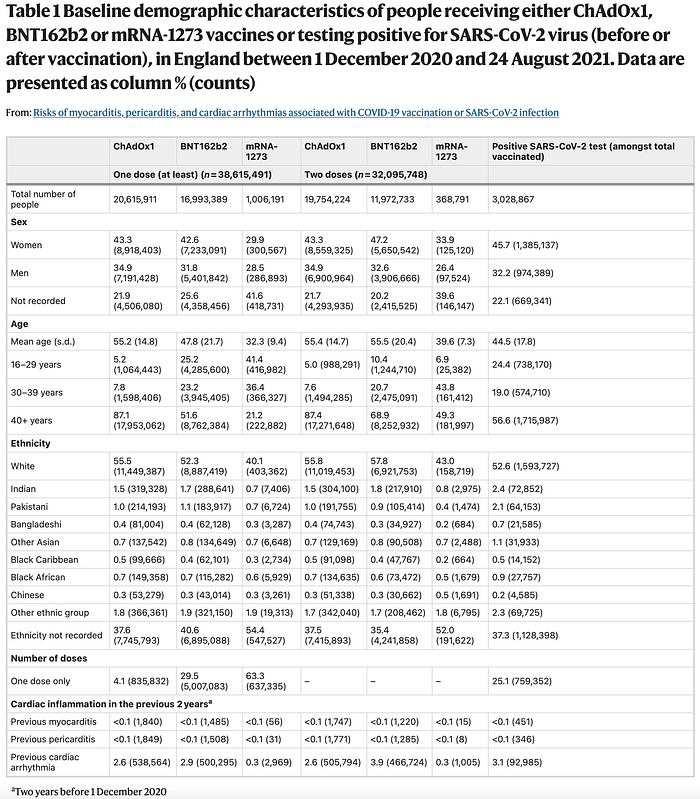
“The outcomes in this study are selected cardiac conditions with previous indications of association with SARS-CoV-2 infection or COVID-19 vaccination. These included myocarditis, pericarditis and arrythmia. We used the International Classification of Diseases-10 codes to define each outcome, as listed in Supplementary Table 11. The outcomes were identified as the first hospital admission due to the event of interest, or death recorded on the death certificate with the International Classification of Diseases-10 code related to the outcome of interest within the study period” the study notes.
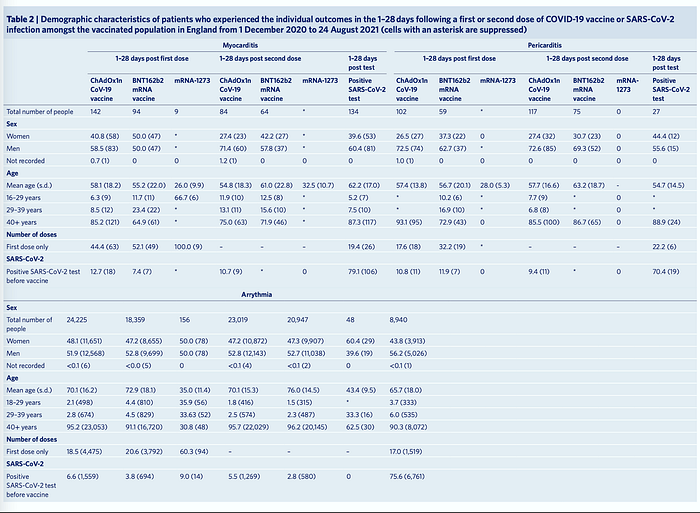
During the study period there were 1,615 and 1,574 admissions or deaths related to myocarditis and pericarditis, respectively (14 patients had both), and 385,508 related to cardiac arrhythmias. Patient characteristics of those who experienced outcomes are enumerated in Table 2 (better visualized in original paper). Notably, of the 38,615,491 vaccinated individuals 1,615 (0.004%) were admitted to hospital with, or died from, myocarditis at any time in the study period (either before or after vaccination); 397 (0.001%) of these occurred in the 1–28 days post any dose of vaccine. Of the 1,615 who were admitted or died, 359 (22.2%) had a SARS-CoV-2 positive test, with 287 (17.8%) of these being before vaccination. There were 114 deaths with myo- carditis recorded on the death certificate as a cause of death (23 had a SARS-CoV-2 positive test). Of those who have been admitted with, or died from, myocarditis in the 1–28 days postvaccination, 12.7% (18) and 10.7% (9) had a positive SARS-CoV-2 test before the first and second dose ChAdOx1 vaccine, respectively, and 7.4% (7) before the first dose of BNT162b2 vaccine.
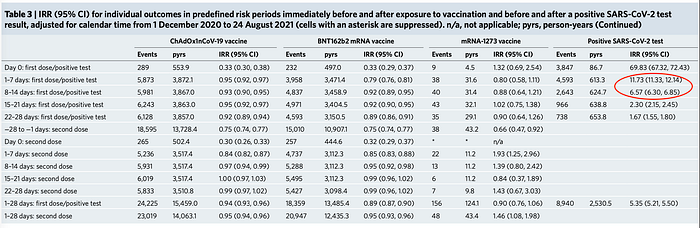
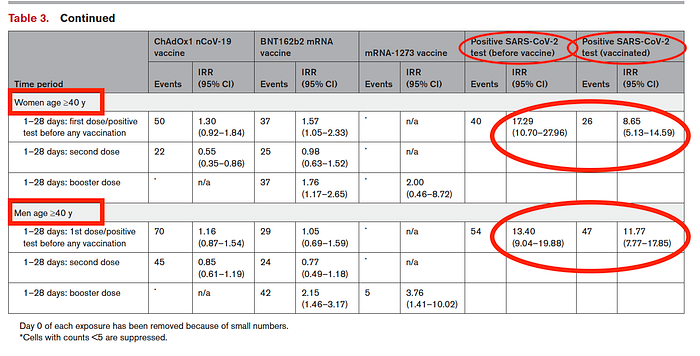
Prima facie, the Incident Rate Ratio (IRR) of myocarditis after COVID-19 infection seems to be greater than after vaccination (Table 3).
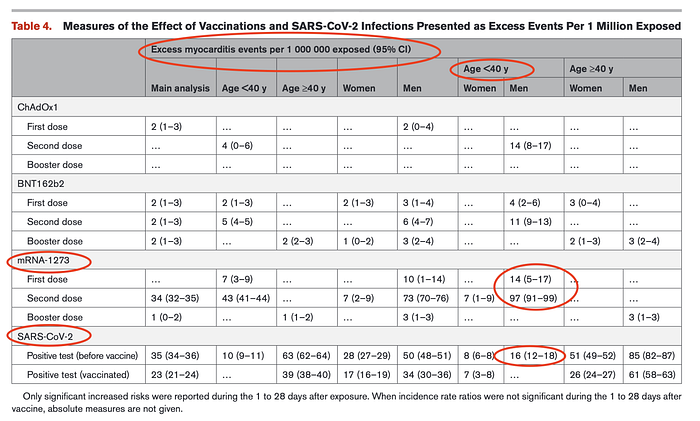
However, separating those under 40 years old from those over 40 years old (Table 4) demonstrates the risk of infection versus vaccination is about the same for those under 40 years old. For those over 40 years old the risk of myocarditis after infection is considerably greater. This should come as no surprise since COVID-19 morbidity and mortality increases dramatically with advancing age. The median hospital duration of stay for those with myocarditis in the 28 days postvaccination was 3 days for ChAdOx1, 3 days for BNT162b2 and 4 days for mRNA- 1273, with means of 8.3, 5.7 and 4.5 days, respectively.
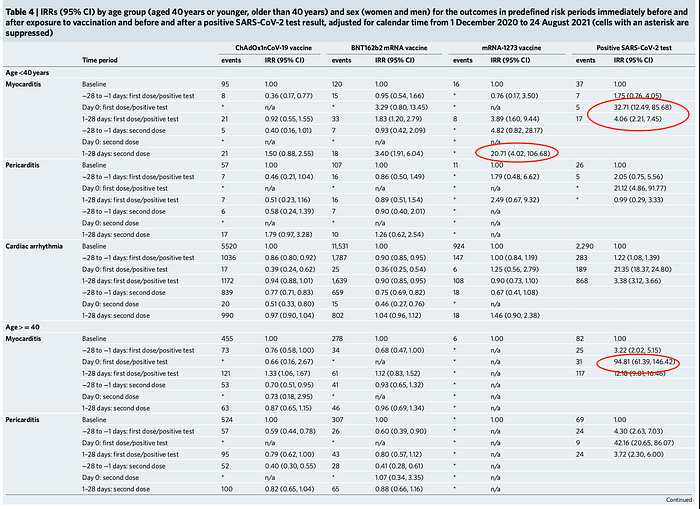
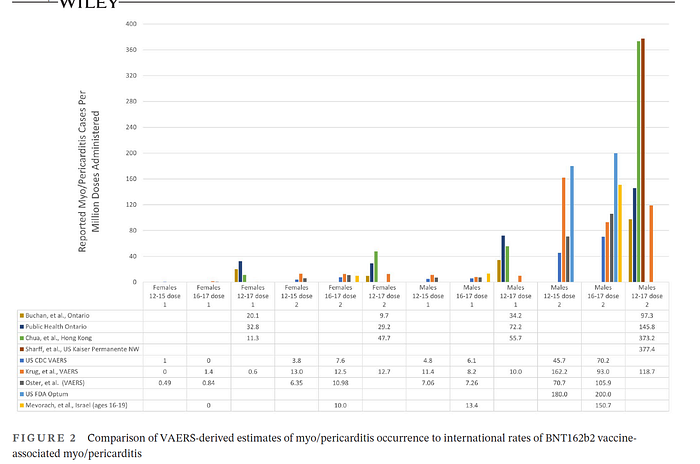
Figure 2 (below) demonstrates how combining all ages obfuscates the increased risk of VAM to younger people, especially after dose 2 of mRNA-1273 COVID-19 vaccination.
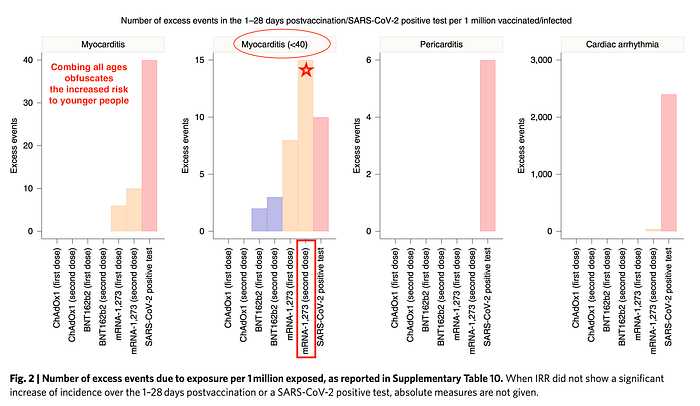
Based upon aggregate analysis (of all age groups), the study authors note: “We estimate that the absolute number of excess myocarditis events in the 28 days following a first dose of adenovirus or mRNA vaccine is between one and six per million persons vaccinated, and the excess risk following the second dose of the mRNA-1283 vaccine is ten per million. By contrast, we estimate 40 excess myocarditis events per million in the 28 days following SARS-CoV-2 infection.” (emphasis mine). The authors erroneously conclude that the risk of myocarditis is greater after infection, overlooking the increased risk of VAM in younger people (and the associated very low risk of severe COVID-19 infection in this same cohort).
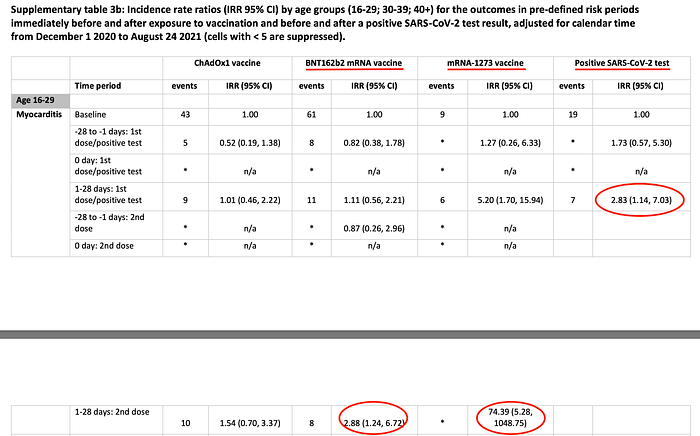
Buried in Table 3b of the Supplementary Appendix is further risk stratification for those 16–29 year old. This analysis reveals that the risk of myocarditis after dose 2 of BNT1262b2 (IRR 2.88) is comparable to that after COVID-19 infection (IRR 2.83). However, the risk of myocarditis after dose 2 of mRNA-1273 is far greater than after infection (IRR 74.39)
As the authors acknowledge, the study is limited by reliance on hospital ICD diagnostic codes (which may over or under estimate the count). Additionally, the study is not designed to assess those who may have died of myocarditis prior to hospitalization. As previously noted, there are reports of autopsy proven myocarditis after COVID-19 vaccination. Additionally, one study over 10 years of autopsied patients with diagnosis of myocarditis, found 57% had sudden death (i.e., of those who dies of myocarditis, 57% had sudden death). Myocarditis accounts for about 6% of Sudden Deaths in Young Competitive Athletes.


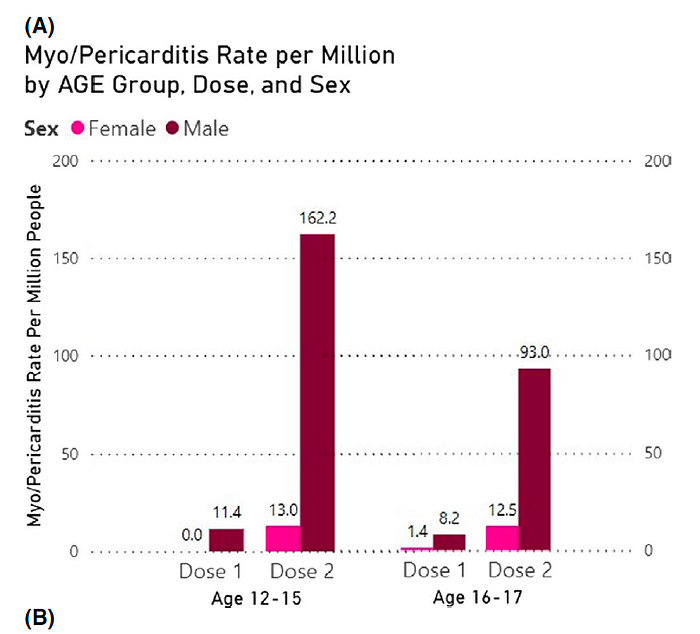
While CDC seemed recalcitrant to publish subgroup analysis until much later, this was the first study to perform stratified risk-benefit analysis of the VAERS data CDC was allegedly closely monitoring and analyzing. The study identified BNT162b2 myo/pericarditis occurrence according to CDC criteria (which itself is restrictive and will be discussed elsewhere in a separate article). Main outcomes were : 1) post-vaccination myo/pericarditis crude incidence in adolescents aged 12–15 and 16–17; and 2) two risk-benefit analyses by age, sex, comorbidity, variant and history of infection. For boys aged 12–15, the rate per million after dose two was 162.2/million or 1/6200. Among boys aged 16–17, our estimate was 93.0/ million or 1/10,800.
Reminder, that VAERS under estimates the risk of myocarditis after vaccination. Subsequent large scale studies with more active surveillance report incident rates greater than300/million after dose 2 of mRNA-1273 COVID vaccination.
Unlike CDC’s erroneous risk-benefit calculation which does not adjust for seroprevalence data, this study did adjust accordingly. Their analysis found that the risk of myocarditis after COVID-19 vaccination may actually be greater than the risk of COVID+ hospitalization in adolescent males.
The study was limited by analysis of BNT126b2 vaccination and the authors acknowledge that the risk is greater after mRNA-1273 vaccine, especially dose 2. Additionally, as this is an analysis of VAERS data, the analysis does not include cases of myocarditis after vaccination that were not reported to VAERS.
In a follow-up study in Circulation (American Heart Association’s prestigious flagship journal), Patone et al. (same lead author as the study from England above), performed a more comprehensive subgroup analysis. This follow-up study analyzed people ages 13 years or older vaccinated for COVID-19 in England between December 1, 2020, and December 15, 2021 for the association between vaccination and myocarditis, stratified by age and sex (previous study did not stratify by sex).
Between December 1, 2020, and December 15, 2021, there were 42 842 345 people vaccinated with at least 1 dose of ChAdOx1 (n=20 650 685), BNT162b2 (n=20 979 704), or mRNA-1273 (n=1 211 956) (Table 1). Of these, 39 118 282 received a second dose of ChAdOx1 (n=20 080 976), BNT162b2 (n=17 950 086), or mRNA-1273 (n=1 087 220), and 21 242 629 people received a third vaccine dose: ChAdOx1 (n=53 606), BNT162b2 (n=17 517 692), and mRNA-1273 (n=3 671 331). The authors do not discuss why 3 724 063 people did not receive the second dose after the first dose. Did they suffer severe adverse reactions? Did some of them die?
Among people receiving at least 1 vaccine dose, 5 934 153 (13.9%) tested positive for SARS-CoV-2, including 2 958 026 (49.8%) before their first vaccination. Of the 42 842 345 people in the study population, 2861 (0.007%) were hospitalized or died from myocarditis during the study period; 345 (<0.001%) patients died within 28 days from a hospital admission with myocarditis or with myocarditis as cause of death recorded in the death certificate. A total of 617 (0.001%) of these events occurred 1 to 28 days after any dose of vaccine (Table 2). Of the 524 patients admitted to the hospital with myocarditis in the 1 to 28 days after any first or second vaccine dose, 151 (28.8%) had received a booster dose: 34.4% (79/230) of those who had ChAdOx1 in the first or second dose and 29.7% (72/243) of those who had BNT162b2 in the first or second dose (Table 2). Of the 5 934 153 patients with a SARS-CoV-2 infection, 195 (0.003%) were hospitalized or died with myocarditis in the 1 to 28 days after the positive test; 114 (58.5%) of these events occurred before vaccination (Table S2).
Notably, in the study period, they observed 140 and 90 patients who were admitted to the hospital or died of myocarditis after a first and second dose of ChAdOx1 vaccine, respectively. Of these, 40 (28.6%) and 11 (12.2%)‚ respectively, died with myocarditis or within 28 days from hospital admission. Similarly, there were 124, 119, and 85 patients who were admitted to the hospital or died of myocarditis after a first, second, and third dose of BNT162b2 vaccine, respectively. Of these, 22 (17.7%), 14 (11.8%), and 13 (15.3%) patients died with myocarditis or within 28 days from hospital admission. Last, there were 11, 40, and 8 patients who were admitted to the hospital for myocarditis after, respectively, a first, second, and third dose of mRNA-1273 vaccine. None of these patients died with myocarditis or within 28 days from hospital admission with myocarditis (Table 2).
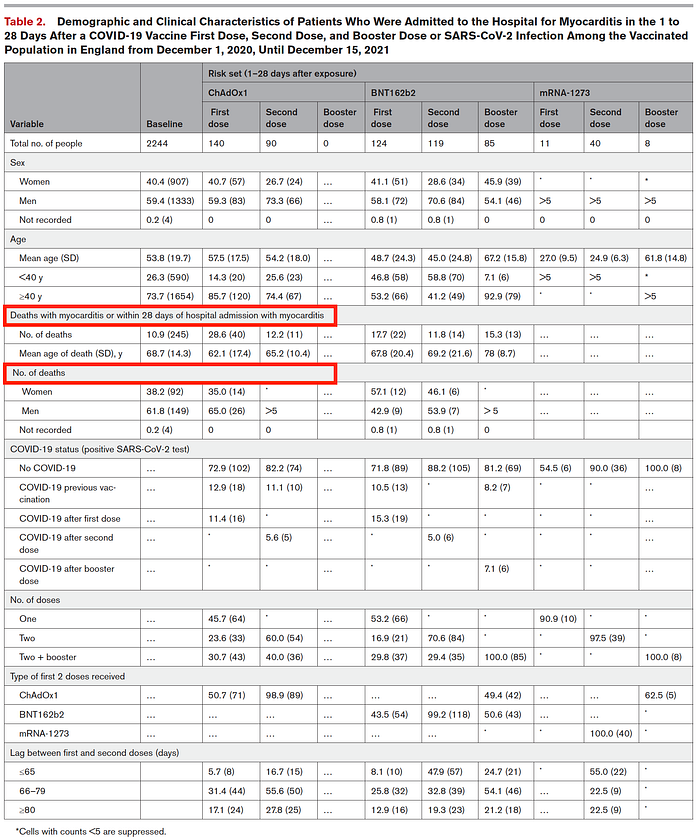
Note: CDC continues to state that VAM cases are “generally mild” and has thus far not acknowledged of deaths due to myocarditis after COVID-19 vaccination. However, this study clearly demonstrates the myocarditis after COVID-19 vaccination can have a considerable mortality rate. (Note: in a separate forthcoming post I will explore in great detail the poor follow-up by by CDC of myocarditis case reports in VAERS; however, the second half of this recent post illustrates the extent to which many are lost to follow-up and may hav actually died).
Subgroup analysis: Men
Of the 17 918 020 men vaccinated in England in the study period, 6 158 584 (34.4%) were younger than 40 years, and 11 759 436 (65.6%) were 40 years or older. Analysis of younger men age younger than 40 years revealed an increased risk of myocarditis after a first dose of BNT162b2 (IRR, 1.85 [95% CI, 1.30– 2.62]) and mRNA-1273 (IRR, 3.06 [95% CI, 1.33–7.03]); and a second dose of ChAdOx1 (IRR, 2.73 [95% CI, 1.62–4.60]), BNT162b2 (IRR, 3.08 [95% CI, 2.24–4.24]), and mRNA-1273 (IRR, 16.83 [95% CI, 9.11–31.11]). The risk of myocarditis for older men 40 years or more was associated with a booster dose of both mRNA vaccines, BNT162b2 (IRR, 2.15 [95% CI, 1.46–3.17]) and mRNA- 1273 (IRR, 3.76 [95% CI, 1.41–10.02]) (Table 3).
Subgroup analysis: Women
Of the 20 979 754 women vaccinated in England in the study period, 7 201 472 (34.3%) were younger than 40 years, and 13 778 282 (65.7%) were 40 years or older . Analysis of women younger than 40 years showed an increased risk of myocarditis after a second dose of mRNA-1273 (IRR, 4.75 [95% CI, 1.11– 20.40]). BNT162b2 was not associated with myocarditis for women under 40 years old. For women 40 years or older, there was an increased risk of myocarditis associated with a first (IRR, 1.57 [95% CI, 1.05–2.33]) and third (IRR, 1.76 [95% CI, 1.17–2.65]) dose of BNT162b2 vaccine. To the best of my knowledge, this is the first study to demonstrate a statistical assocation of myocarditis after vaccination in women also.
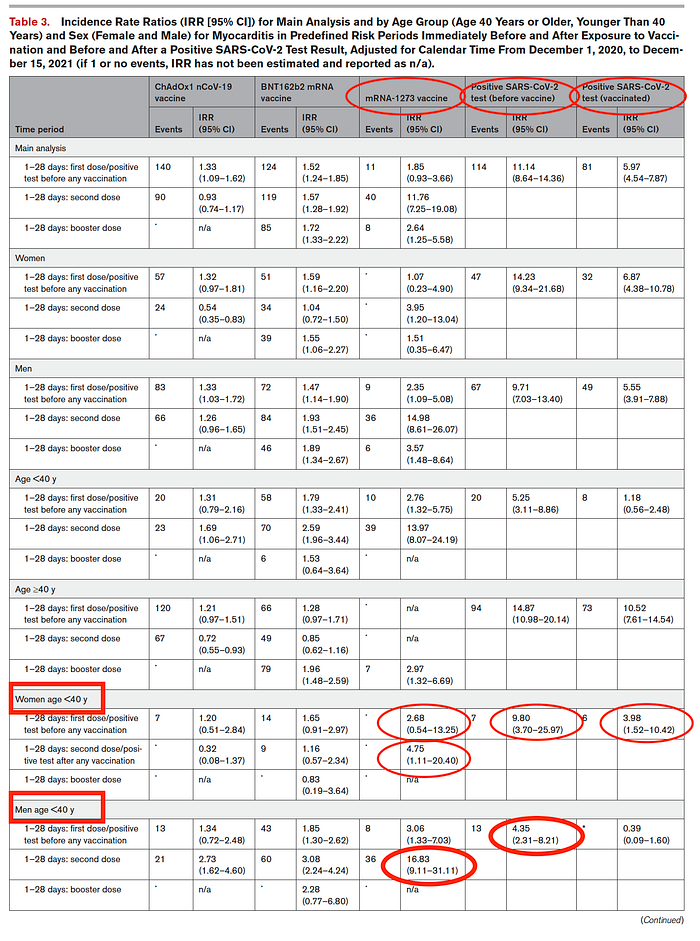
However, for both men and women over 40 years old, the IRR of myocarditis is greater after COVID-19 infection than after COVID-19 vaccination.
Excess deaths per million vaccinations or COVID-19 infections were also assessed by the study. Again, for males under 40 years old, the excess cases of myocarditis were far greater after COVID-19 vaccination than after COVID-19 infection. It is worth pointing out that excess cases of myocarditis after BTN126b2 vaccination were comparable to myocarditis cases after COVID-19 infection for those under 40 years old, but considerably lower than after infection for those over 40 years old.
Accidental Neglect or Intentional Omission?
Conspicuously, absent from the discussion is subgroup analysis for those 16–29 years old. Recall that in the original study by these same authors, subgroup analysis for those 16–29 years old demonstrated a striking increased IRR after dose 2 of mRNA-1273 (74.39!). Surely the authors are aware of this finding in their own paper, especially since numbers studies in the interim have demonstrated increased rate of myocarditis after COVID-19 vaccination in adolescents and young adults (reviewed in detail here).
Limitations
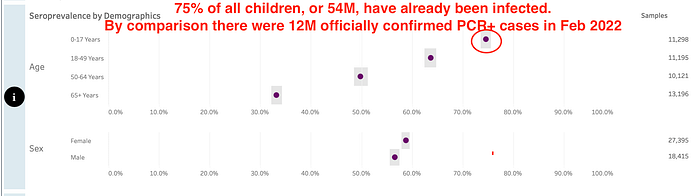
The study is limited in several ways. First, as discussed above, 3 724 063 people did not receive the second dose after the first dose. These could reflect severe adverse reactions, deaths, or change in attitude toward vaccination. Whatever the reason, this ought to have been discussed by the authors. Secondly, the study is reliant on hospital ICD diagnostic codes, which the authors admit could under or over estimate the events of myocarditis. Thirdly, the study cannot account for those who may have died of myocarditis prior to hospitalization. Finally, in their assessment of the COVID-19 infection events, the authors do not seem to adjust for seroprevalence data. Here in the US, seroprevalence data from CDC suggests far more people have been infected with SARS-CoV2 than officially confirmed PCR+ ‘cases’ (75% of all children have already been infected as of February 2022). This would very significantly change the calculation for risk of myocarditis from SARS-CoV2 infection. The risk and benefit analysis needs to use a representative denominator on both sides for accurate comparison of true risk.
The American Heart Association’s review of this study reaches a very different conclusion (ignoring most of the limitations I discuss above), concluding the benefits outweigh the risks for most people (though they do acknowledge the increased risk of myocarditis after vaccination in males under 40 years old). I am referencing their review for full transparency and comparision.
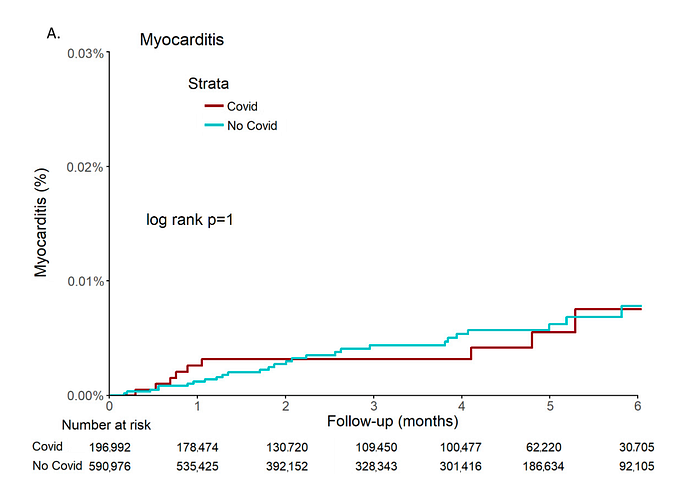
In a retrospective cohort study of 196,992 adults after COVID-19 infection in Clalit Health Services members in Israel between March 2020 and January 2021 patients were followed for six months. “Inpatient myocarditis and pericarditis diagnoses were retrieved from day 10 after positive PCR. The control cohort of 590,976 adults with at least one negative PCR and no positive PCR were age- and sex-matched.” The study population has 27% obesity, whereas obesity prevalence in US is 42%. Thus caution must be applied in generalizing this study to US population.
The study found age (aHR 0.96; p =0.045) and the male sex (aHR 4.42; p = 0.003) were independently associated with myocarditis. Obesity was borderline associated with myocarditis (aHR 2.31; p = 0.053). Most notably, COVID-19 infection was not associated with myocarditis (aHR 1.08; 95% CI 0.45 to 2.56, p = 0.869). This study supports the interpretation above that findings from CDC MMWR ought to be adjusted seroprevalence data (i.e., infection cohort denominator needs to be adjusted by 4.5 times to account for the seroprevalence data). Without the adjustment for seroprevalence data, CDC erroneously concludes that myocarditis after SARS-CoV2 infection occurs at a greater rate than after vaccination.
SUMMARY
Myocarditis after COVID-19 vaccination and SARS-CoV2 infection continues to be a topic of tremendous public health interest. Passive surveillance such as data from VAERS seriously under estimates this risk. Risk stratified analysis by age and sex reveals the risk in young males is far greater after vaccination than after infection. The risk of myocarditis after SARS-CoV2 infection is very real and seems to be greater in people over 40 years old. In this older group, the risk of SARS-CoV2 infection may be greater. However, all such analyses included earlier variants of the virus, which has demonstrated progressively decreased virulence with each subsequent variant. The original Wuhan strain was especially virulent and the more recent Omicron variant seems to be much less virulent. Most estimates of the myocarditis after COVID-19 vaccination do not adjust the denominator for seroprevalence data, mostly using officially confirmed ‘cases’ based upon PCR+ testing. Most studies do not account for those who may have died of myocarditis prior to hospitalization. Such analysis is glaringly absent and made difficult by obliterating the control arm of the Phase III trials.
School and college vaccine COVID-19 vaccine mandates are using incorrect risk-benefit analyses and perpetrating mandated preventable harm. This is an egregious affront to medical ethics. As the full extent of the long term implications are finally understood, it may be nothing short of crimes against humanity.
