These Recent Studies Further Underscore Ethical Concerns About COVID-19 Vaccination in Children

BACKGROUND

SARS-CoV2 is a virus with significantly different morbidity and mortality for healthy children and young adults than for elderly and those with underlying medical conditions. For the elderly, symptomatic disease causing COVID-19 pneumonia carries high morbidity and mortality. Per CDC mortality data, 75% of all COVID+ deaths have been in those over 65 years old. This older cohort also comprises almost 50% of all COVID+ hospitalizations. CDC analysis of COVID+ hospitalizations found 91% had at least one underlying medical condition. For the elderly, in-hospital COVID-19 mortality has been as high as 30%. Indeed, the morbidity and mortality in the elderly is considerable. Our efforts to mitigate their morbidity and mortality has tremendous scientific, epidemiological and moral justification.

For healthy children and young adults, SARS-CoV2 tells a different tale. The pediatric population comprises about 0.1% of all COVID+ deaths, with an infection fatality rate (IFR) of about 0.0018%. Hospitalization rate is probably much less than 0.7% noted by American Academy of Pediatric data based upon officially confirmed PCR+ infections. This study and this study previously found that 40% of pediatric COVID+ hospitalizations may have been over estimated (when differentiating those hospitalized for COVID-19 pneumonia versus those who were hospitalized for other causes but had incidental COVID+ testing during routine surveillance). Adjusting for this potential 40% over estimation, the hospitalization rate may be 0.42% of children infected with SARS-CoV2. However, that doesn’t complete the needed adjustments to the crude data. CDC seroprevalence data report 75% of all children have already been infected (4.5 times more than officially confirmed PCR+ results). With this additional adjustment, perhaps the actual true SARS-Cov2 hospitalization rate for children then is as low as 0.09%. This study estimated the risk of hospitalization in pediatric population to be 0.22%

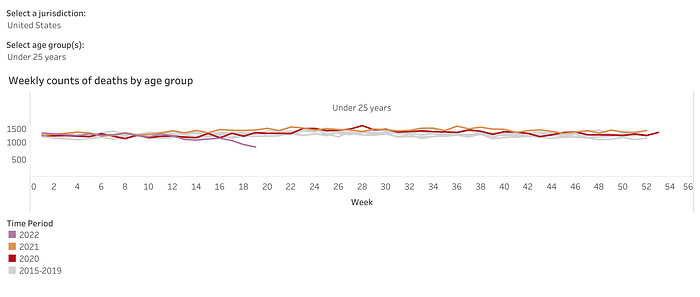
In-hospital COVID+ mortality for children has consistently been less than 3%. Per CDC COVID+ mortality data, those less than twenty-five years old comprise 0.34% of all COVID+ deaths. Most notably, there were zero excess deaths in 2020 and 2021 compared to prior years for the those less than twenty-five years old. This begs the question: was there ever an emergency amongst children and young adults warranting Emergency Use Authorization (EUA) for COVID-19 vaccines, let alone school and university vaccine mandates?
COVID-19 VACCINE EFFECTIVENSS IN CHILDREN
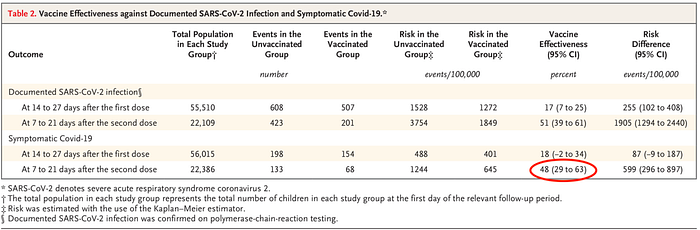
Using a large health care database, a recent study from Israel assessed the vaccine effectiveness (VE) against Omicron variant for BNT162b2 COVID-19 vaccination in children 5–11 years old. Those with evidence of prior SARS-CoV2 infection (by PCR, antigen, or serology) were excluded. The study found VE for symptomatic infection to be 48% 7–21 days after second dose. Previously, a smaller US study found VE in children declined from 60% to 29% from first to second month after second dose of BNT162b2 COVID-19 vaccination. Therefore, if this Israeli study were to follow the children beyond 21 days, the VE would almost definitely be even lower than 48%.
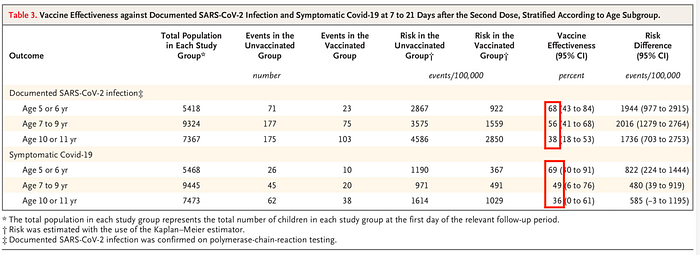
Also, as the authors note, assessment of “vaccine effectiveness against more severe outcomes such as hospitalization were not possible, because they were very rare in the study population.” With such low incidence of COVID+ hospitalizations in pediatric population (as noted above, probably as low as 0.09%), many trials were not large enough to detect a statistically significant difference in COVID+ hospitalizations or deaths between vaccinated and unvaccinated children.
There are some noteworthy limitations of this Israeli study. 17% of the children were obese or overweight. By comparison, data from NIH indicate 35% of children in US are overweight or obese. 43% of study population had received at least three doses of influenza vaccine in the past five years. In US, an estimated 58% of children receive annual flu vaccine. Therefore, caution must be exercised in applying the results of this Israeli study to US population.
An additional limitation of this study is the number of children who did not receive the second dose. The authors note “many of the children in our study cohort did not receive a second dose within the study follow-up period.” The percent of study population that did not receive the second dose is not mentioned in the study or the supplementary appendix. Details of the size of this subset would be helpful because the size could significantly influence the interpretation of the results. mRNA COVID-19 vaccinations have a known and demonstrable risk of myocarditis and other rare severe adverse reactions. To better contextualize the risk-benefit analysis it would be helpful to know how many did not receive the second dose and the reason why they did not.
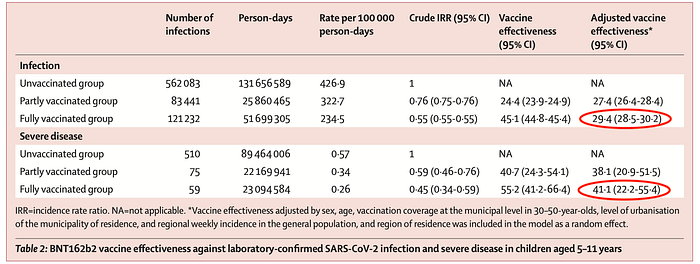
Another recent study from Italy, linked data from national COVID-19 surveillance system and national vaccine registry to evaluate efficacy of COVID-19 vaccination in children 5–11 years old. By April 3, 2022, 35.8% of all children 5–11 years old had been vaccinated. During the study period, there were 766,756 cases of SARS-CoV2 infection and 644 cases of severe COVID-19 (627 hospitalizations, 15 admissions to intensive care unit, and two deaths). No details are provided on percent of study population with obesity or other underlying medical conditions, therefore generalizability to our population must be done with caution. Furthermore, 134,386 children were only partially vaccinated (did not complete vaccination series after one dose). As noted above for the study from Israel, the reasons why they did not complete the vaccination series could better inform the risk-benefit analysis. With these limitations in mind, the study found VE in the fully vaccinated was 29% against infection and 41% against severe COVID-19. VE against infection decreased to 21% 43–84 days after full vaccination. As the authors note, this is in stark contrast to the high VE touted in the original trials leading to EUA: “Our estimates of the effectiveness of full vaccination against SARS-CoV-2 infection are significantly lower than those reported in the clinical trial that led to the approval of BNT162b2 in children (90.7% in the approval trial vs 29.4% in our study).” [Invited commentary to this Italian study can be found here.]
RISKS OF COVID-19 VACCINE ASSOCIATED MYOCARDITIS (VAM)
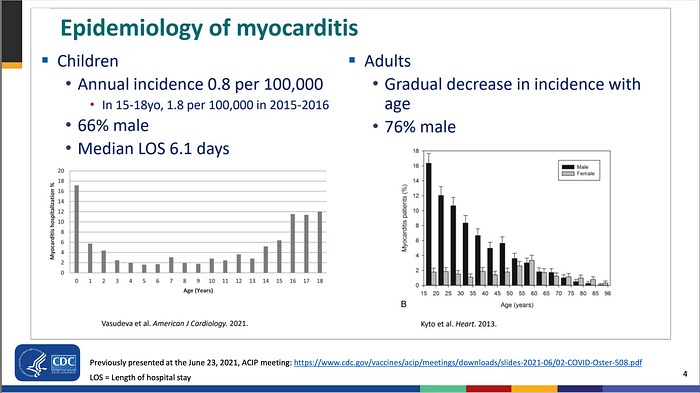
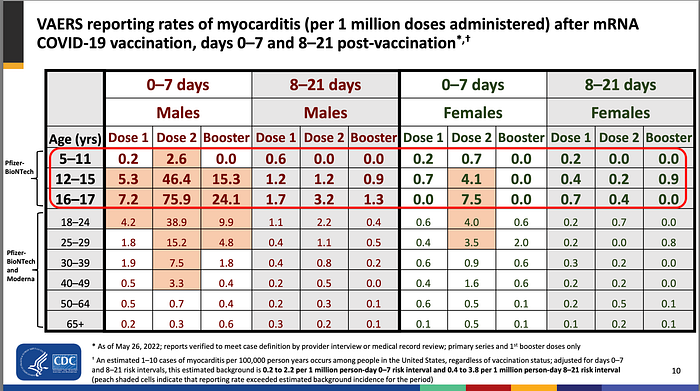
mRNA COVID-19 vaccinations are not without their risks. During the June 23, 2022 meeting of CDC’s Advisory Committee on Immunization Practices (ACIP), an Update on myocarditis following COVID-19 vaccination notes the background annual rate of myocarditis in children to be 8 cases per million (0.8 per 100,000). The presentation primarily focuses on VAERS data, yielding a rate of 75 cases per million after mRNA COVID-19 vaccination.
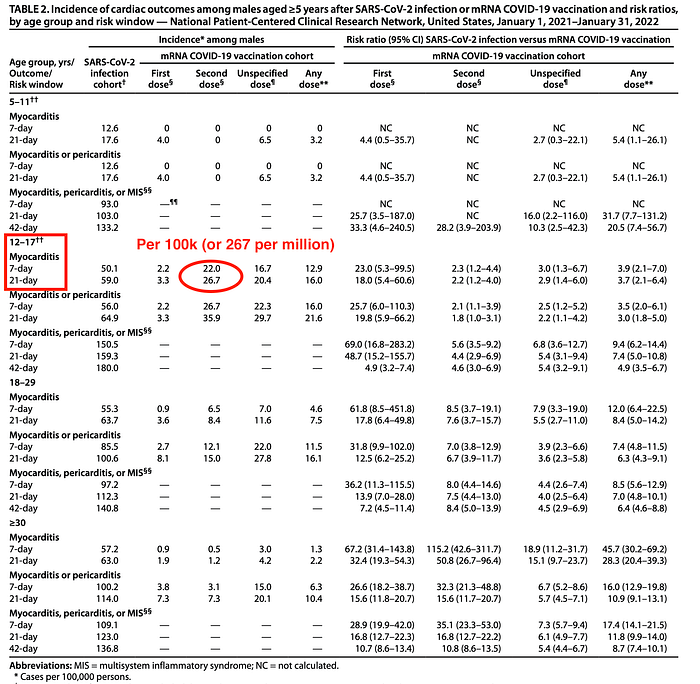
However, CDC’s own MMWR on myocarditis which analyzed data from 40 health care systems found a rate of 267 cases of myocarditis per million (12–17 year-old children).
Additionally, in the Summary Bases of Regulatory Action (for Moderna’s mRNA COVID-19 vaccination), they note:
“analysis of VAERS data from passive surveillance indicated a reporting rate of 40 cases per 1 million second doses administered to males 18 to 24 years of age, while an FDA meta-analysis of four healthcare claims databases in CBER’s Biologics Effectiveness and Safety System estimated a rate of 148 cases per 1 million males 18 to 25 years of age vaccinated with the 2-dose primary series.”
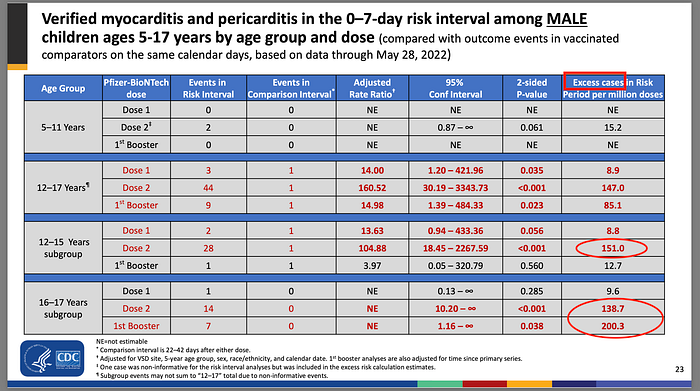
Knowing that analysis of health care system data yields a rate of 3–4 times higher than VAERS, one wonders why CDC’s ACIP continue to emphasize VAERS data in their risk-benefit analysis presentations. Unlike VAERS which is based upon passive reporting and is known to under estimate the risk of myocarditis, the Vaccine Safety Datalink (VSD) is a collaborative project between CDC and 9 integrated healthcare organizations. Compared to expected cases of myocarditis, the VSD analysis at the June 23rd meeting, found an excess cases of 151 per million for 12–15-year-old children. For 16–17-year-old children, VSD analysis found 138 per million excess cases, but that jumped to 200 excess cases per million after the first booster.
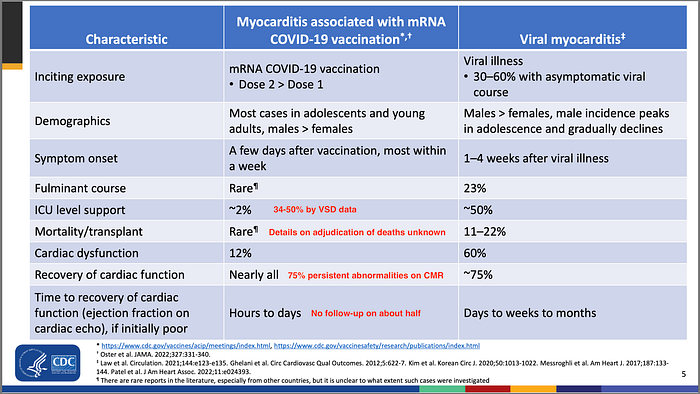
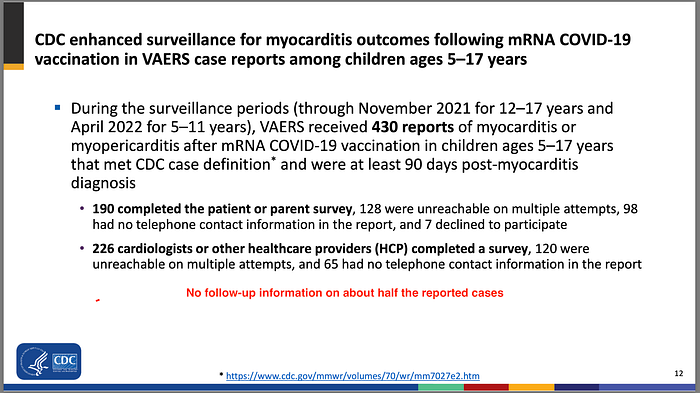
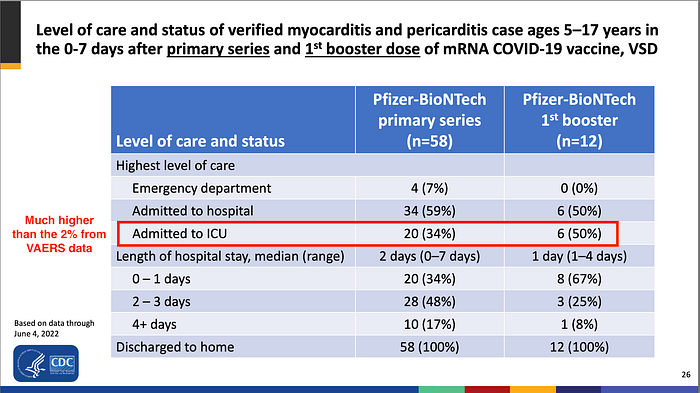
While CDC continues to emphasize that most cases of myocarditis have been mild, it is important to note that their analysis does not include those who may have died before being hospitalized. Furthermore, they have follow-up information on only about half of the myocarditis cases reported in VAERS. Why were the other half lost to follow-up? Did they have a serious decline in clinical condition? How many of them died? Although CDC’s analysis suggests 63% had fully recovered at 90-day follow-up, previous cardiac MRI study found 75% had persistent abnormalities on cardiac MRI at 3–8 months follow-up. CDC’s analysis of VAERS data suggests only 2% of myocarditis cases (after COVID19 vaccination) needed ICU level support, but using VSD data that jumps to 34% after primary vaccination and 50% after the booster. Repeatedly, active surveillance reveals a higher rate of myocarditis after vaccination and more a severe disease course than VAERS data alone.
SUMMARY
Repeated studies have demonstrated much lower VE than the 90% touted by the original trial data. Despite real world data, especially with Omicron, revealing a much lower VE, Public Health officials have not updated their projections of COVID+ hospitalizations and deaths averted by mass vaccination programs. Furthermore, reliance upon VAERS alone has been repeatedly shown to under estimate the true risk of myocarditis when compared to more active surveillance of insurance and health care database analyses. The overall risk-benefit of COVID-19 vaccination in children does not seem to be favorable and most certainly does not warrant school and university vaccination mandates. In fact, Sweden decides against recommending COVID vaccines for kids aged 5–11. “With the knowledge we have today, with a low risk for serious disease for kids, we don’t see any clear benefit with vaccinating them,” Health Agency official Britta Bjorkholm told a news conference. Certain subgroups of high risk children and young adults may indeed benefit from COVID-19 vaccination. However, categorical school and university mandates seem deeply problematic because of the subsequent medical harm that will likely ensue. Despite this, CDC continues to recommend COVID-19 vaccination in all children 6 months and older.