Myocarditis after vaccination against COVID
Why mandated COVID vaccination polices in schools and universities are unethical

Federal officials advising the Centers of Disease Control and Prevention met on Wednesday June 23rd to explore the possible link between myocarditis (inflammation of the heart muscle) and the mRNA Emergency Use Authorization (EUA) COVID vaccines by Pfizer and Moderna. “The facts are clear: this is an extremely rare side effect, and only an exceedingly small number of people will experience it after vaccination,” said a statement co-signed by the Department of Health and Human Services, the CDC and 15 medical, public health and provider organizations. Although they did find an increase risk of myocarditis after vaccination, they noted the events are extremely rare, usually resolve on their own, and the vast majority generally did very well after complete recovery from the symptoms. They therefore concluded everyone should continue to receive the EUA COVID vaccines, including adolescents 12 and over. Almost as soon as the decision was announced an Opinion piece was published in the Washington Post, declaring “The benefits of vaccination in young adults far outweigh the risks, including for myocarditis”. The favorable analysis offered by the CDC and by the Washington Post opinion piece bely the underlying flaws in their methodology.
CASE DEFINITION
Using self-generated reports from Vaccine Adverse Event Reporting system (VAERS), CDC report identified 484 total preliminary reports of myocarditis or pericarditis through June 11, 2021. Of those, 323 met the CDC working case definition of myocarditis or pericarditis (or both). CDC’s case definition for “confirmed myocarditis” requires diagnosis with cardiac MRI or heart muscle biopsy. Many community hospitals in the US do not have cardiac MRI available. A biopsy is usually only performed in tertiary care centers with advanced heart failure or transplant specialists. Unlike our European counterparts, biopsy is seldom if ever performed for myocarditis unless it is a severe case necessitating aggressive interventions. Thus, any myocarditis report in VAERS from a hospital without cardiac MRI or biopsy capabilities would be excluded from the confirmed case count and analysis. Also, 148 of 484 reports in VAERS are still under review. Given the potential gravity of the problem, the review of these 148 remaining reports ought to have been completed prior to the CDC’s meeting on June 23, 2021.
In contrast to the CDC’s case definition, as the table below demonstrates, cardiology practice guidelines do not necessitate cardiac MRI or biopsy for a “probable acute myocarditis” diagnosis.

A person with “cardiovascular symptoms” and at least one of the other criteria (biomarkers of cardiac injury, EKG findings suggestive of cardiac injury, or abnormal function of either echocardiogram or cardiac MRI) can be diagnosed with “probable acute myocarditis” clinically. A “definitive myocarditis” diagnosis is given with heart muscle biopsy, which is usually only performed in severe cases.
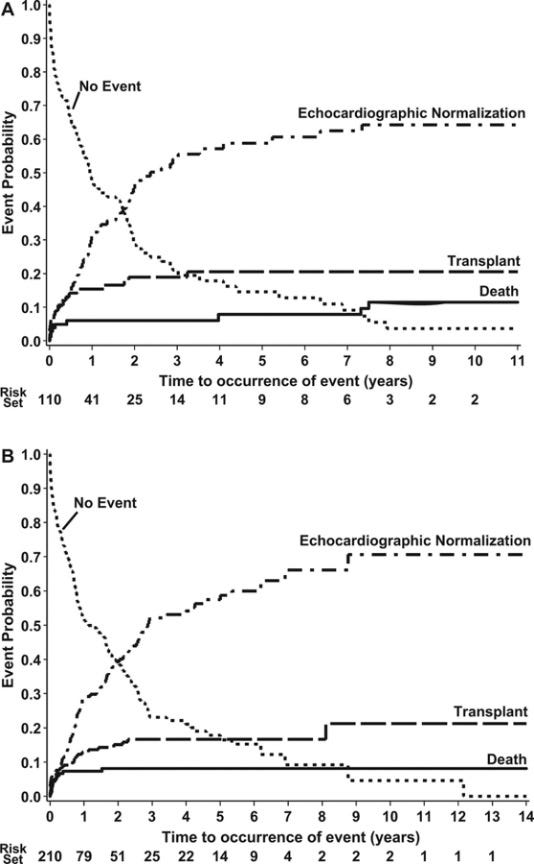
Whether acute myocarditis is diagnosed clinically (with symptoms and an echo or MRI) or diagnosed by biopsy, the outcomes are comparable (in the graph below Figure A shows outcomes of myocarditis diagnosed by biopsy and Figure B shows outcomes of myocarditis diagnosed clinically).
UNDERESTIMATING THE RISK USING VAERS
Israel Health Ministry’s data on myocarditis after vaccination indicates the risk to be 1in 3,000 to 1 in 6,000. Unlike the CDC which relies upon self-reporting in VAERS, Israel’s analysis was based upon active surveillance of nationwide health records. There is no scientific justification to assume that the incidence of myocarditis after vaccination in Israel would be dramatically higher than the incidence in the US. US federal officials could commission a study of insurance health care records to more comprehensively assess incidence of post vaccination myocarditis. A recent study assessing association between social gatherings and COVID risk using birthdays, did precisely that (“cross-sectional study used nationwide data from January 1 to November 8, 2020, from 2.9 million US households with private insurance”) — that approach is not impossible for researchers motivated to perform a more comprehensive and accurate review.
Underestimation of the risk by passive surveillance using only VAERS is not just a hypothetical concern. The CDC estimates that 2.5–11 per million doses result in anaphylaxis after EUA COVID vaccination. However, a study employing active surveillance found the rate of anaphylaxis after EUA COVID vaccination to be about 247 per million doses (22 times higher than the upper limit of the CDC’s estimate). Another study evaluating risk of myocarditis after small pox and influenza vaccination also utilized active surveillance, concluding that passive surveillance significantly underestimates the true incidence of myocarditis and pericarditis after vaccination Therefore, sufficient justification exists to suspect the CDC’s estimate of incidence of myocarditis after EUA COVID vaccination is grossly underestimated also.
OUTCOMES AND PROGNOSIS
In their analysis, the CDC concludes that most myocarditis cases had complete recovery. Of the 323 “confirmed cases”, 309 were hospitalized, 295 of which were discharged. Of these 295, 218 (79%) are “known to have recovered from symptoms at time of report”, and 9 are still hospitalized (2 of which are in ICU). Information of outcomes is unavailable for 5 of them. While the CDC emphasizes that the vast majority recover quickly, the analysis overlooks the importance of the 21% that did not yet have complete resolution of symptoms at time of report. For those who have complete recovery within weeks, myocarditis has a very favorable long-term prognosis. However, prolonged hospitalization with ongoing symptoms or ICU stay can indicate more severe disease, which increases the risk of dilated cardiomyopathy and the need for heart transplant. Studies on long term prognosis after acute myocarditis are mostly limited to five-year follow-up.
Cardiovascular complications of pediatric myocarditis can include sudden death. One study over 10 years of autopsied patients with diagnosis of myocarditis, found 57% had sudden death. Myocarditis accounts for about 9% of sudden death in young athletes in the United States. It can also lead to arrhythmias, even in the absence of left ventricular dysfunction. Myocarditis may mimic a heart attack. A study of pediatric patients presenting with myocarditis and a chest pain found that all had elevations of cardiac troponin I (biomarker of heart injury, with peak range 6.54–64.59 ng/mL) in the presence of normal values of inflammatory markers. The prognosis was good with resolution of cardiac abnormalities within a few weeks, similar to the adult experience. Of those who develop dilated cardiomyopathy, a meta-analysis found that 58% have recover with favorable prognosis. The remaining 42% are at increased risk of ongoing heart failure, chronic dilated cardiomyopathy, sudden cardiac death, and ultimately may even need heart transplant. A study of hospitalized myocarditis patients in the United States found that nearly half of the patients required blood pressure support, 37.5% required mechanical ventilation, and 7.4% required extracorporeal membrane oxygenator (ECMO) support. Fulminant myocarditis (a distinct subset characterized by sudden heart failure and hemodynamic compromise) has been described in children with mortalities varying from 48.4% in Japan to 9% in France. The risk of death and heart transplantation persists up to 12 years after diagnosis of acute myocarditis in children.
Finally, animal models have shown an association with sustained aerobic exercise and increased risk of death.Because of this and the known association of myocarditis with sudden death in young athletes, current guidelines from the 2005 Bethesda Conference for activity with acute myocarditis recommend activity restriction from competitive athletics and other vigorous exercise for at least 6 months. A return to training and competition is possible if heart function is normal and there are no clinically relevant arrhythmias.
COMPARING TO COVID MYOCARDITIS
COVID also causes severe complications, including myocarditis. Citing one study, Leana Wen in her Washington Post Opinion piece Wednesday, mistakenly notes that 2.3% of nearly 1600 collegiate athletes had myocarditis. This certainly grabs attention. However, a careful review of the study demonstrates that of the 37 athletes who were diagnosed with COVID myocarditis, 9 had symptoms of myocarditis but 28 had no symptoms of myocarditis at all. Furthermore, 20 of the cases were deemed “possible” myocarditis, whereas only 8 were “probable” myocarditis. By comparison, the CDC’s case definition includes only symptomatic myocarditis confirmed by cardiac MRI. Several studies of COVID myocarditis young adults have been published, all of which conduct active surveillance (screening all qualifying persons in the study with cardiac MRI). By contrast, the CDC’s analysis depends solely upon passive surveillance (voluntary reports in VAERS). The preponderance of published evidence the incidence of symptomatic COVID myocarditis indicates it is much less than the 2.3% mentioned in the cited study, which includes symptomatic and asymptomatic, possible and probable cases of COVID myocarditis. Finally, severe COVID complications in adolescents and young adults tend to occur more often in those with underlying medical problems like diabetes, obesity, or congenital circulatory problems. In contrast, myocarditis after vaccination seems to be occurring in individuals without underlying medical problems. The two groups have different risk profiles and ought to be analyzed differently. Recognizing this difference in risk profiles, a German panel gave limited approval for COVID vaccine only for high-risk adolescents. Sweden also recommends COVID vaccination only for high risk children.
LOW RISK IS NOT THE SAME AS MANDATED RISK
Much of the public health rhetoric on myocarditis after vaccination emphasizes the low risk and that it is “very rare”. This constant refrain glaringly overlooks the ethics of mandated risk. Not everyone who is exposed to a person with the virus SARS-CoV2 will become infected, let alone develop any symptoms. In one study, 72% of health care workers did not develop any serological evidence of infection even after direct exposure to a patient with COVID in a hospital setting without a mask. With reasonable mitigation efforts like ventilation and wearing high-quality masks, the risk of infection can be significantly curtailed and is by no means mandated. With current case counts in US so low, the risk of becoming infected with random exposure is indeed very low. But after vaccination, there is almost 100% chance of generating an immune reaction (and thereby incurring risk of myocarditis at a rate of 1 in 3,000 to 1 in 6,000 children and young adults) Despite this, many schools and universities are considering mandated COVID vaccination policies for students. Mandated risk is ethically different than low risk, especially since the risk of myocarditis after vaccination is greatest in those with the lowest risk of severe COVID complications themselves.